An antagonist is a drug that has an affinity for a receptor but zero efficacy (intrinsic activity of zero)
Competitiveness
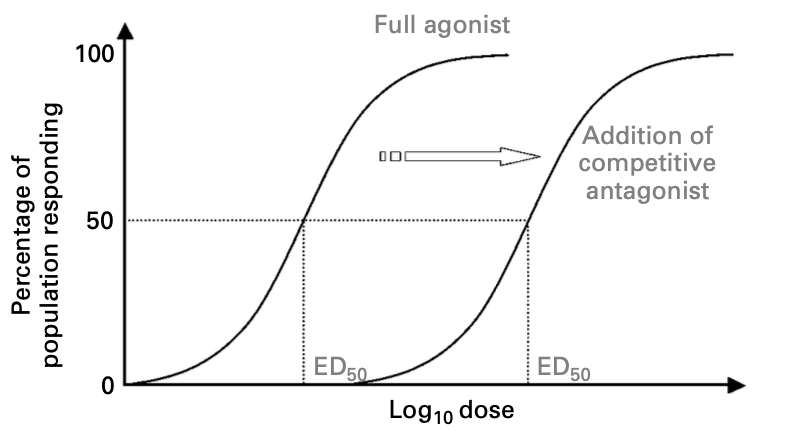
Competitive antagonists compete with the endogenous agonist for the same binding site
They can be reversible or irreversible
There are multiple examples, including non-depolarising NMBAs or β-blockers
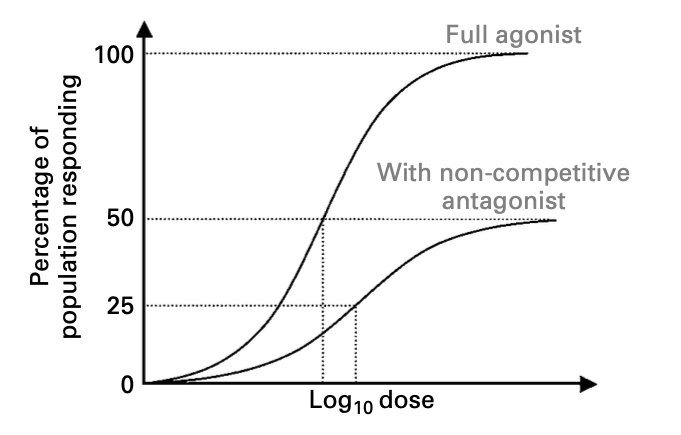
Non-competitive antagonists bind at a different site on the receptor to the natural agonist, causing a conformational change in the receptor to prevent its activation
For example, ketamine is a non-competitive antagonist of glutamate at the NMDA receptor
Reversibility
Reversible antagonists - the inhibitory effect of the antagonist can be overcome by increasing the concentration of agonist e.g. non-depolarising NMBA, naloxone, phentolamine
Irreversible antagonists - the inhibitory effect of the antagonist cannot be overcome by increasing the agonist concentration e.g. aspirin, clopidogrel
Allosteric modulators
Allosteric modulators bind at a different site to the natural ligand, altering the affinity of the receptor for the ligand, which may increase or decrease the effect of the natural agonist
E.g. benzodiazepines at the GABAA receptor
Adapted from Physics, Pharmacology and Physiology for Anaesthetists
The effect of the antagonist can be overcome by increasing the concentration of the agonist
As such, if there is a competitive antagonist present, the log dose-response curve of a full agonist is shifted to the right (higher ED50) in a parallel fashion
Adapted from Physics, Pharmacology and Physiology for Anaesthetists
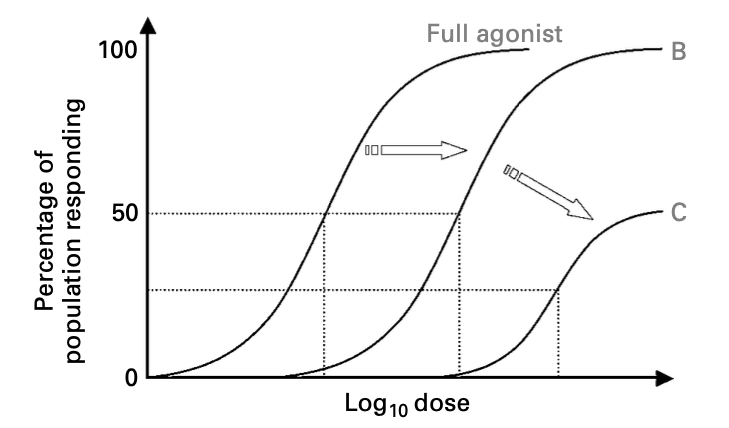
Maximal agonist response (100% efficacy) is still possible at low antagonist levels if enough agonist is added, at the expense of reduced potency (increased ED50; Line B)
This is because of receptor redundancy
However, with increasing antagonist levels, a maximal response cannot be achieved no matter how much agonist is added (Line C):
Adapted from Physics, Pharmacology and Physiology for Anaesthetists
The non-competitive antagonist induces a conformational change in the receptor and so the agonist cannot bind
Increasing the dose of agonist is not fruitful as there are no more available receptor sites available (i.e. receptor redundancy is moot because the agonist will bind to the receptor but can't activate it)
The curve is similar to that of a partial agonist, with:
Reduced efficacy (sub-maximal response)
Lower potency (increased ED50, curve shifted to right in a non-parallel fashion)
Reduced gradient of curve
The dose ratio is the factor by which the agonist concentration must be increased, in the presence of a competitive antagonist, in order to produce an equivalent response
Dose ratio = Dose of agonist in the presence of a competitive antagonist / Dose of agonist in the absence of a competitive antagonist
pA2
The affinity of an antagonist for a receptor is known as the pA2
It is the negative logarithm in base 10 of the concentration of antagonist that requires a doubling of the dose of agonist to achieve the same response
I.e. -log10[antagonist] to give a dose ratio of 2
Physiological antagonism describes when drugs act on opposing physiological mechanisms
Examples include:
Fentanyl (respiratory depressant) and doxapram (respiratory stimulant)
Ritodrine (tocolytic beta-blocker) and oxytocin (uterotonic)
Furosemide and amiloride
Does not include pharmacological antagonism e.g. opioid + naloxone
Pindolol (non-selective beta blocker with partial beta agonist activity, also partial agonist/antagonist activity at 5-HT1A receptor)