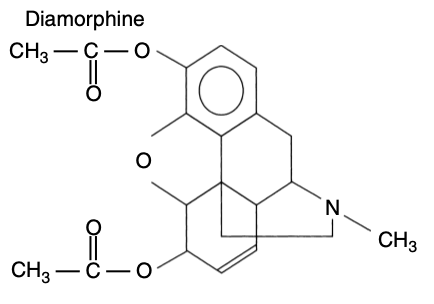
- Diamorphine is an ester, a di-acetylated morphine derivative with a potency 2x that of morphine
- It is a pro-drug with no affinity for opioid receptors - active metabolites are responsible for its effects
- As with all opioids it is a weak base
- Tablets are available but not in the UK
- A white powder containing 5mg, 10mg, 30mg, 100mg or 500mg of the hydrochloride salt, which is dissolved to form a solution for administration
- Largely an analgesic, although can be used to treat dyspnoea e.g. in palliative care settings
- Neuraxial doses:
- Intrathecal: 300-400micrograms
- Epidural: 1-3mg
- pKa 7.6
- 37% unionised at pH 7.4
- Reduced oral bioavailability due to extensive 1st pass metabolism
- Has a relatively high lipid solubility and therefore is well absorbed from the GI tract and can be used effectively by a SC route
- Has a higher lipid solubility than morphine, therefore
- Diamorphine has a more rapid onset than morphine
- Has a shorter duration of action
- Is less likely to cause (late) respiratory depression than morphine
- 40% plasma protein bound
- Volume of distribution: 350L
- Plasma half-life 5mins
- Undergoes ester-hydrolysis by plasma and tissue esterases in the liver, plasma and CNS
- Active metabolites are morphine and 6-monoacetylmorphine, which are both MOP receptor agonists
- 50-60% of an administered dose appears in the urine as morphine derivatives
- 0.13% is excreted unchanged
- Elimination half-life 3mins
- The clearance of the morphine component is 3.1 ml/min/kg
- Largely similar to morphine/that of a typical opioid
- Produces significantly more euphoria than other opioids, hence its place as a drug of abuse (heroin)