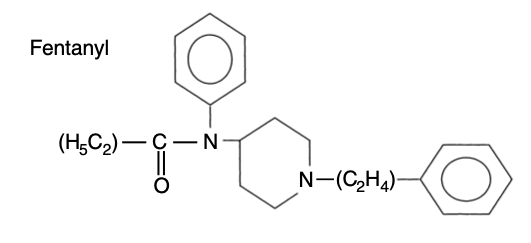
Fentanyl is a synthetic phenylpiperidine derivative
As with all opioids, it is a weak base
Presentation
A clear, colourless solution of 50micrograms/ml stored at room temperature in a controlled drug cupboards, in glass vials of 2ml or 10ml volume
Transdermal patches which release 25-100μg/hr for 72hrs
Lozenges and lollipops which release 200μg-1.6mg over 15mins, for buccal use
Uses
Short-term analgesia for acute nociceptive pain
Approximate dose of 1-2μg/kg, but ultimately titrated to effect
Obtund the cardiovascular response to laryngoscopy
As a (co-)induction agent as part of a 'cardiac stable'induction
Large doses are required e.g. 500-1,000μg (approximately 50-100μg/kg)
Procedural sedation, typically alongside a hypnotic agent, in small doses e.g. 50-75μg
As a neuraxial opioid alongside local anaesthetic
Epidural: standard infusion regimens contain 2μg/ml fentanyl; boluses of 50-100μg for top-ups
Intrathecal: 10-25μg
As an infusion
Usually to maintain sedation and analgesia on critical care
Although pharmacokinetic models for target-controlled infusion exist (McClain, Shafer) they are not commercially available
Molecular weight: 286
Water solubility: 1:30 - 1:100 i.e. not very water soluble vs. morphine
Lipid solubility (logP at pH 7.4): 2.3 i.e. significantly more lipid soluble than morphine
Skin flux: 1 i.e. significantly better skin flux than morphine
Absorption
pKa 8.4
Only 9% unionised at pH 7.4
Relative lipid solubility vs. morphine: 600x
Therefore rapid onset of action
As high lipid solubility causes less respiratory depression
Distribution
83% plasma protein bound
Volume of distribution 4L/kg (high)
At <3μg/kg IV its short duration of action is due to its distribution
Following prolonged administration or high doses, its duration is significantly prolonged as tissues become saturated
E.g. doses of 50-100μg/kg have a duration of approximately 6hrs
This is reflected in its context-sensitive half-times
At 1hr (20mins CSHT) and 3hrs (70mins CSHT) it is fairily similar to alfentanil
However at 8hrs of infusion, fentanyl's CSHT (260mins) is significantly longer than alfentanil's (60mins)
May become trapped in the stomach; 99.9% ionised in an acidic environment
Becomes unionised in the alkaline small bowel and is absorbed
Metabolism and excretion
Rapid hepatic 1st pass metabolism
Metabolism is primarily to norfentanyl (via N-demethylation) which undergoes further hydroxylation
Inactive metabolites are excreted in the urine
Pharmacokinetics reflect high lipid solubility and volume of distribution:
Clearance is 13ml/min/kg
Elimination half life 190mins
Primarily an MOP receptor agonist, although does have some action at KOP receptors too
100x more potent than morphine
Anaphylactic reactions are rare but can occur if the tertiary amine group becomes a quaternary amine (e.g. in vials where the citrate preservative runs out, or after the ligand has bound to the opioid receptor