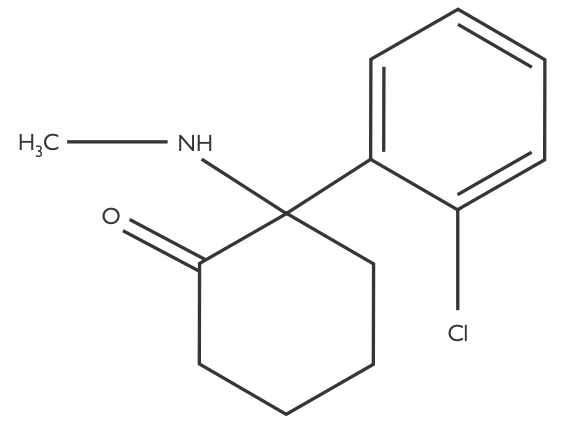
- Ketamine is a phencyclidine derivative that exerts its anaesthetic effect predominantly through non-competitive antagonism of the NMDA receptor
- Does not induce anaesthesia in one arm-brain circuit time
- It has a molecular weight of 238g/mol
- IV (1-2mg/kg) - onset 30-90s and duration 5-10mins
- Nasal
- IV via PCA, either alone or mixed with an opioid
- Epidural
- Sub-anaesthetic IV dosing
- 10-20mg single bolus
- 0.25mg/kg bolus or 0.25mg/kg/hr infusion
- IV e.g. 10-20mg boluses titrated to effect
- IM (4-10mg/kg) - onset 2-8mins and duration 10-20mins [NB pain on injection]
- PR (10mg/kg)
- PO
- Bronchodilatory properties so may be used in refractory asthma/bronchospasm
- Clear colourless solution with a pH of 4.5
- Concentrations of 10mg/ml, 50mg/ml or 100mg/ml, stored in glass vials at room temperature
- Presents as either:
- A racemic mixture of the inactive, R(-) enantiomer and the active, S(+) enantiomer
- Combined with 1-in-10,000 benzethonium chloride preservative, which is neurotoxic
- An enantiopure preparation of S(+) ketamine
- Preservative free therefore safe for use in epidurals
- Relatively expensive
- Much greater (4x) affinity for the NMDA receptor and 2-3x more potent than the R(-) enantiomer
- Responsible for the cardiovascular effects of racemic ketamine (BJA, 2021)
- It has a pKa of 7.5
- Bioavailability
- IM: 93%
- Epidural: 77%
- Intranasal: 45-50%
- Sublingual: 25-30%
- Rectal: 25-30%
- Oral: 20%
- Volume of distribution is 3L/kg although this is increased in critically ill patients
- 25% protein binding
- Described using 2- and 3-compartment models and suitable for use as a TCI e.g. the Domino, Hijazi or Clements models
- Hepatic metabolism - total body clearance dependent on hepatic blood flow
- Phase I → CYP450 enzymes (2B6, 3A4) to the weakly active metabolite norketamine (1/3 as potent)
- Phase II → glucuronidation to inactive metabolites
- Metabolites excreted in the urine (91%)
- Clearance 17ml/kg/min
- Elimination half life 2-3hrs
- Unchanged respiratory drive (BJA, 2025 (1), BJA, 2025 (2))
- Preserved laryngeal reflexes
- Is a bronchodilator via histamine antagonism and bronchial smooth muscle relaxation
- There is increased muscle tone in the jaw that may precipitate obstruction
- It can cause sialorrhoea and bronchorrhoea, which can predispose children to obstruction/laryngospasm
- Reduces neuronal catecholamine uptake, leading to:
- Increased heart rate, cardiac output and therefore blood pressure
- Increased myocardial work and oxygen consumption
- Raised pulmonary vascular resistance (but not SVR)
- As such ketamine is relatively contraindicated in those with myocardial ischaemia
- S(+) ketamine may be preferable in IHD as it produces less cardiac depression (although does induce some direct myocardial depression)
- Doesn't block ATP-sensitive K+ channels, which is a key mechanism of ischaemic myocardial preconditioning
- Non-competitive NMDA receptor antagonism by binding to the allosteric site
- Reduces presynaptic glutamate release
- This produces dissociative anaesthesia
- Dissociates thalamo-neocortical and limbic systems
- There is δ and θ activity on EEG; the ɑ-rhythm is abolished
- Intense analgesia
- Thought to reduce opioid tolerance by blocking action of PSD-93/-95 proteins
- Demonstrates some μ-antagonism but κ- and σ- partial agonism
- Intense amnesia
- Vivid, unpleasant dreams, hallucinations and delirium (5-30%)
- Can occur for up to 24hrs post-dose
- Reduced by concurrent use of opioids or BZD's
- Same frequency but reduced intensity by using S(+) ketamine
- Less common in: paediatric, elderly, those less to recover undisturbed
- Also causes antagonism at nicotinic ACh, muscarinic ACh and mono-aminergic receptors
- Local anaesthetic activity at high doses via action on neuronal Na+ channels
- Historically thought to increase cerebral blood flow, CMRO2 and ICP
- Subsequent work has not replicated this
- There's a lack of evidence supporting these purported deleterious effects of ketamine in brain injury or increased ICP
- Increases IOP although not in a clinically meaningful fashion
- Sialorrhoea
- Increased frequency of PONV vs. propofol and thiopentone
- Interstitial cystitis with high-dose, non-prescription use (Class C drug of abuse)
- Unsafe in porphyria