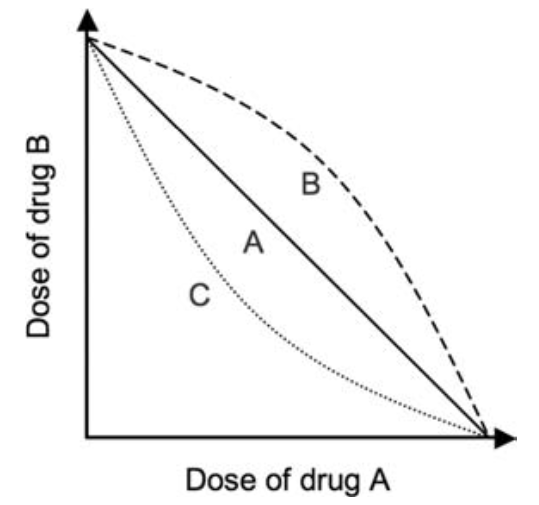
Summation
- The actions of two drugs are additive, but each has an independent action of its own e.g. midazolam and propofol
Potentiation
- The action of one drug is amplified by the second drug, which has no separate action of its own
- For example, magnesium's effect on NMBA at the nAChR at the NMJ
- E.g. probenecid reduces the renal excretion of penicillin
Synergism
- The action of the two drugs is greater than would be expected from a purely additive effect
- E.g. remifentanil and propofol
- E.g. sulphonamide antibiotics and trimethoprim; both are bacteriostatic but when given together become bactericidal
- E.g. clonidine and opioids
Antagonism
- The action of the two drugs is opposing
- E.g. flumazenil and benzodiazepines (direct effect)
- E.g. neostigmine and non-depolarising NMBA's (indirect effect)