- Rapid sequence induction i.e. where rapid, profound neuromuscular blockade is required
- Facilitate intubation for short surgical procedures or those where only brief blockade is desired (e.g. surgical requirement for facial or recurrent laryngeal nerve monitoring)
- To reduce muscle twitching associated with electro-convulsive therapy
Suxamethonium
Suxamethonium
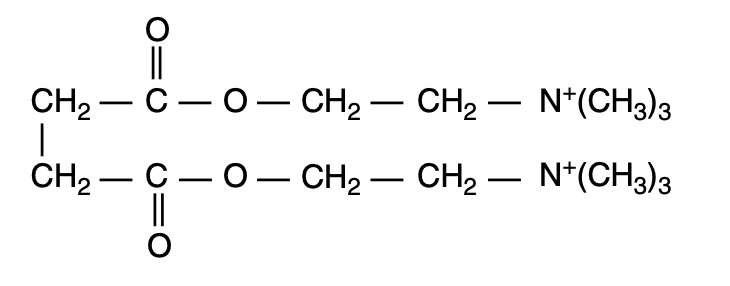
- Suxamethonium (succinylcholine) is a depolarising NMBA comprising of two acetylcholine molecules joined back-to-back via their acetyl groups:
- Other depolarising agents from the 'methonium' family, although not used in UK practice, include:
- Decamethonium
- Suxethonium
Presentation
- Presents as a clear, colourless solution of its chloride salt
- Concentration of 50mg/ml
- Stored at 4ºC (i.e. in the fridge)
Dosing
- IV: 1 - 1.5mg/kg (not affected by age)
- Onset of action within 30s and determined by the end of fasciculations
- Duration 3-5mins
- IM: 2 - 4mg/kg (typically reserved for paediatric patients)
- Binds the nAChR causing membrane depolarisation
- Its hydrolysing enzyme (plasma cholinesterase) isn't present at the NMJ therefore suxamethonium has a duration of action longer than native acetylcholine
- Persistent depolarisation of the receptor initiates local current circuits:
- enders voltage-gated sodium channels within 1-2mm of the receptor inactive
- The area of electrical inexcitability prevents action potential transmission
- This leads to muscle relaxation
- This initial depolarising block is a Phase I block
- Muscle function starts to recover in 5 mins and is complete 15mins post 1mg/kg dose
- If further doses of suxamethonium are given, it may become a Phase II block [i.e. similar characteristics to non-depolarising block, although different mechanism]
Absorption
- Minimal oral bioavailability
Distribution
- Rapid distribution
- 20% protein-bound
- Only 20% of initial IV dose reaches NMJ
- VD = 0.14L/kg
Metabolism
- Rapidly hydrolysed by plasma cholinesterase (plasma and liver)
- Succinylmonocholine is weakly active
Suxamethonium → succinylmonocholine + choline → succinic acid + choline
Excretion
- <10% excreted unchanged in the urine due to rapid metabolism
- Half-life 1-2mins
Cardiovascular
- Arryhthmogenic, especially in paediatric patients
- Stimulation of muscarinic AChR in the sinus node can cause:
- Nodal or sinus bradycardia
- Ventricular arrhythmias
- Bradycardia is often more severe after a second dose
Neurological
- IOP (normally 15mmHg) is raised by 10mmHg for minutes post-suxamethonium dose
- The mechanism is unknown
- ?Transient dilation of choroidal blood vessels
- ?Contraction of tonic myofibrils
- Co-administration of thiopentone will keep IOP static
- This is significant in the presence of globe perforation
- Repeated doses may cause a phase 2 block (this is not more common in neonates)
Gastrointestinal
- Raises intragastric pressure by 10cmH2O
- However there is a simultaneous increase in LOS tone and therefore no increased risk of reflux
Metabolic
- Hyperkalaemia
- There is a small rise in serum potassium as depolarisation causes K+ efflux into the extracellular fluid (0.2 - 0.4mmol/L)
- Patients with neuromuscular disorders or (>10%) burns are susceptible to a sudden release of K+, which may be large enough to cause cardiac arrest
- Extra-junctional AChR (foetal subtype) proliferate over the surface of the muscle
- Paraplegic patients: period of particular risk is in the first 6 months although continues in those with progressive muscular disease
- Neuromuscular disorders including dermatomyositis, dystrophia myotonica and others
- Burns patients: safe for the first 24hrs after thermal injury and from 18 months afterwards
- Renal failure patients are not at increased risk of sudden hyperkalaemia per se, though may already have high K+ levels and therefore be at increased risk
Musculoskeletal
- Myalgia - commonest in young female patients mobilising rapidly post-operatively
- Pre-medication with small doses of diazepam, gallamine (non-depolarising NMBA) and dantrolene have limited effect at reducing myalgia
Adverse reaction